

Abstract
Introduction: Patients (pts) with transformed follicular lymphoma (t-FL) exhibit an aggressive clinical course and high risk of relapse. In this study we have analysed the clinical characteristics, prognostic factors, treatments and survival outcome of pts with pathologically confirmed t-FL.
Methods: We reviewed pts with low grade lymphoma who developed a subsequent aggressive B-cell lymphoma at MDACC from 7/1998 to 07/2017. Transformation was defined as development of an aggressive lymphoma in the setting of a prior diagnosis of low grade NHL. Pts with composite histology or grade IIIb FL at dx were excluded. We identified a total of 273 pts who transformed from a low grade lymphoma, including 172 with an initial diagnosis of FL (63%), MZL (18%), and SLL (19%).Pts with t-FL were analyzed for clinical characteristics, treatments and outcome. Overall survival (OS) was defined from the time of initial diagnosis of t-FL to death/last follow up while failure free survival (FFS) was calculated from time of starting first line treatment after transformation to treatment failure/discontinuation/switch or death. Optimal cut off values for various prognostic markers associated with survival were identified using recursive partitioning.
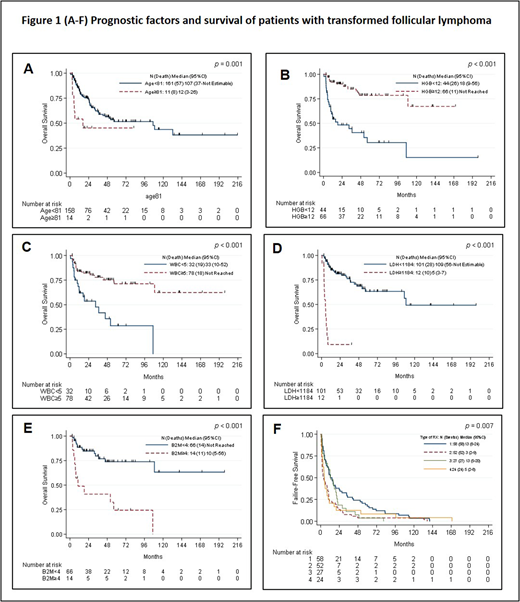
Results: Among the 172 pts with t-FL, 164 (95%) were diffuse large B cell lymphoma (DLBCL) and 8 (5%) with other histology. The median follow up time after transformation was 21.3 months (0.6-215 months). The median age at transformation was 63 (33 to 88) and 59% were males. The median time from initial diagnosis of FL to t-FL was 41 months (2 to 379 months). In the 122 pts where initial grading was available; 47, 43, and 32 were I, II, IIIa, respectively. Median lines of treatment received prior to transformation were 1 (range 0-11) and 124 pts (72%) had prior treatment with rituximab. Thirty one pts (18%) were in observation for FL prior to transformation. B symptoms in 13% pts, 12% has ECOG PS (3-4), CNS involvement was noted in 1% and median number of sites involved at transformation were 1 (range 1-6). 52 pts (30%) had transformation at a site distant from the initial site of FL. Twenty eight of 32 pts (87%) who had MYC testing (by IHC) were positive. Other characteristics included, 41% pts with lambda monoclonal light chain expression, median Ki-67 was 75% (8-100%), LDH > ULN in 47%, MUM-1 + in 56%. Median β2M was 2.3 mg/dL. Overall, the median OS from transformation was 106.7 mo (36.8-Not Estimable) and the median FFS = 8.77 mo (5.6-10.5). There was no survival difference between pts with DLBCL and HD. At the time of last follow up, 107 pts were alive and 65 died, including 45 due to progression. . Overall, 161 pts received treatment for t-FL, 58 with R-CHOP (Rx1), 52 with R-non-CHOP (Rx2), 27 with R-EPOCH based (Rx3), and 24 with miscellaneous treatments (Rx4). In univariate analysis, we identified factors significantly associated with inferior OS, (lower hemoglobin, low platelet counts, lower absolute lymphocyte counts, higher LDH, and higher β2M). Advanced ECOG-PS and presence of B symptoms also correlated with inferior OS. Using recursive partitioning, age ≥ 81 years, Hb < 12 gm/dL, WBC < 5K/uL, LDH ≥1184, β2M ≥ 4 mg/dL were associated with significantly increased risk of death (Figure-1 A-E). In multivariate analysis, age ≥ 81 years (HR=3.95, 95% CI 1.82-8.60; p=0.001), presence of double hit lymphoma (DHL) (HR=4.15, 95% CI 1.74-9.91; p=0.001) and Rx2 treatment (R-non-CHOP based regimen, compared to Rx1, Rx3 and Rx4) (HR=2.36, 95% CI 1.27-4.38; p=0.001) had inferior OS. We also analysed FFS in pts with information available on their initial therapy for t-FL (n=161). Presence of DHL and treatments other than R-CHOP were predictive of inferior FFS in MVA. Pts who received non-CHOP based regimens had inferior FFS (Figure-1F; p=0.007).
Conclusions: Patients with t-FL have a heterogeneous disease course and most pts can be salvaged with subsequent therapies. R-CHOP based regimens appear to have most benefit following transformation. Common laboratory tests hemoglobin, WBC, platelet count, LDH and beta2 microglobin help in predicting the survival of t-FL pts. In pts where MYC was tested, most were positive. Comprehensive cytogenetic and molecular analyses are needed to recognize various pathogenic mechanisms and identify novel therapeutic targets in t-FL.
Nastoupil:Janssen: Research Funding; Karus: Research Funding; Gilead: Honoraria; Novartis: Honoraria; Genentech: Honoraria, Research Funding; Juno: Honoraria; Celgene: Honoraria, Research Funding; Merck: Honoraria, Research Funding; Spectrum: Honoraria; TG Therappeutics: Research Funding. Samaniego:ADC Therapeutics: Research Funding. Westin:Celgen: Membership on an entity's Board of Directors or advisory committees; Apotex: Membership on an entity's Board of Directors or advisory committees; Kite Pharma: Membership on an entity's Board of Directors or advisory committees; Novartis Pharmaceuticals Corporation: Membership on an entity's Board of Directors or advisory committees. Wang:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Consultancy, Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; MoreHealth: Consultancy; Acerta Pharma: Honoraria, Research Funding; Kite Pharma: Research Funding; Juno: Research Funding; Pharmacyclics: Honoraria, Research Funding; Novartis: Research Funding; Dava Oncology: Honoraria. Fowler:Pharmacyclics: Consultancy, Research Funding; Janssen: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal